A good while back -- several months, at least -- I began writing an entry that was based on the contents of my teaching portfolio. That post is still hanging about in draft form, and I will complete it, but there's something about the material that triggers major anxiety, that makes me replace the clunky notebook on the shelf.
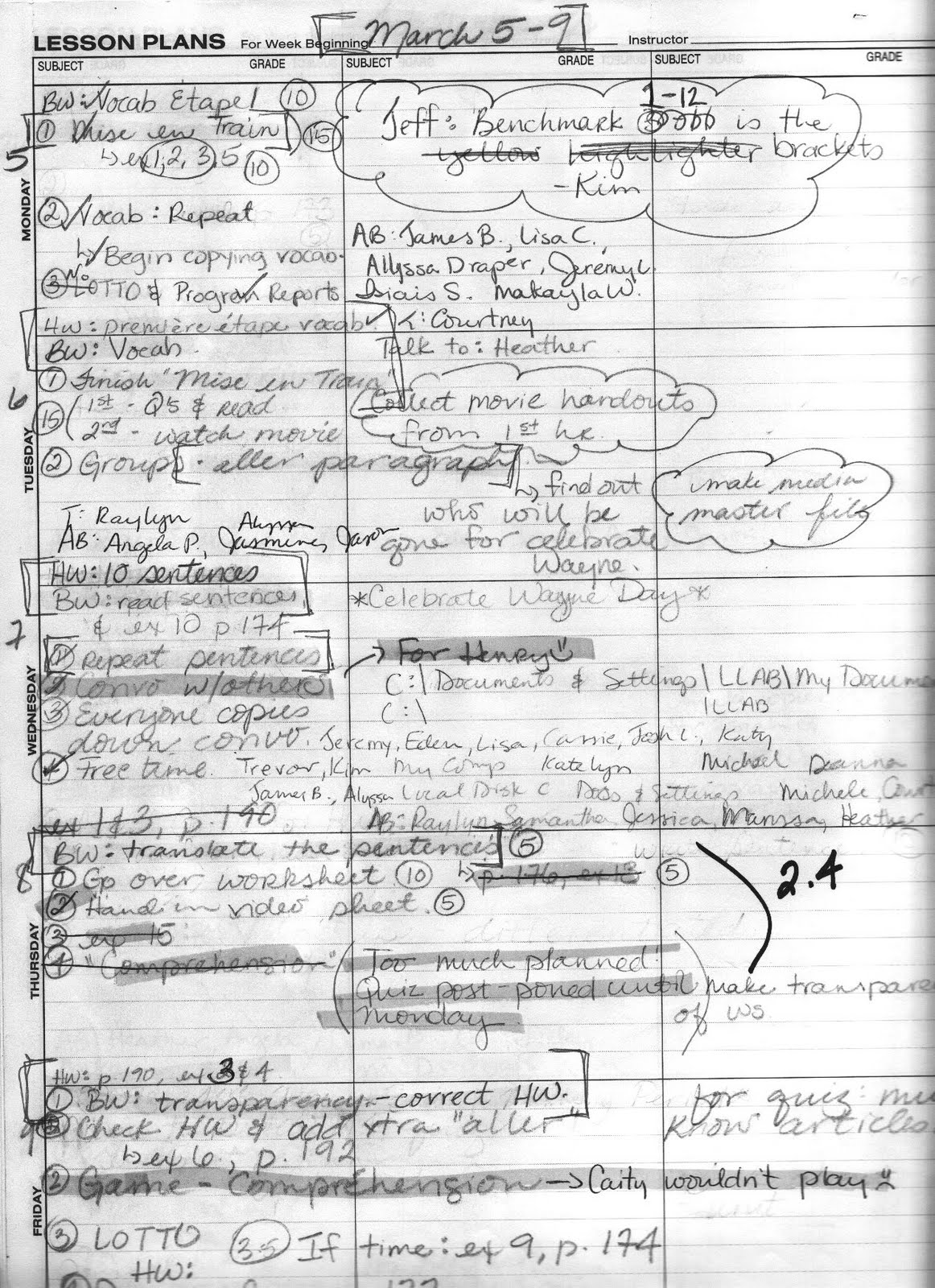
It's as if I am reading the evidence of someone else's life. The memories stimulated by this odd group of documents are, for the most part, happy ones (with the exception of the remembered angst behind every asininely detailed "daily lesson plan"). Some of the entries are there solely to impress the committee evaluating educators by this "instrument." Some of the entries are there solely to irritate that same judgmental group -- like my inclusion of project guidelines for Throw-Away-the-Book Week.
There surely are things hinted at between the white vinyl covers that no sane person would miss. For example, I included the lengthy negative evaluation I received from an administrator who inspected one of my more advanced French classes. She gave me the lowest possible marks for stuff like clarity of instruction, review of home work assignments, and the flow of class exercises -- because all were conducted "in a foreign language," by far, the strangest criticism I ever received.
She was well-known for her negativity. When she came up to me at the close of class, she asked me why some assignment was not written on the board. I pointed out a boxed bit of writing in an upper corner and told her that that was the assignment (again, written in French), to which she responded with a doleful "I guess I have to take your word for it." I should have yelled: "Shazaam! You caught me pulling that old fake assignment trick. Foiled again!"
Okay, so as I tell you about The Portfolio, some of the old rigor returns. I am who I was; I remember me.
A big part of what The Bosses wanted to see involved student evaluations and evidence of "contact" with both student and parents/guardians. This aspect of teaching was really pretty new to me, as my experience until then was with college students. The onus of contact was more on the student in that world, though I did blur the directional road map when it seemed the right thing to do -- when someone was sick, depressed, or radically different from their norm. [This inclination was born with my very first batch of essays to grade. Near the top of the pile was an essay in the form of a suicide note. That surely cemented several good habits in me -- from attempting to return papers as fast as possible to cultivating a positive relationship with Campus Police. Incredibly, this happened once more in my career. How sad to think that I was their only available confidente.]
When I took a job at the high school level, I was clueless about the complexity of student/parent contact work. On paper, scheduling a 30-minute window for phone calls home and disciplinary referrals looked sufficient. In actuality, when I was doing my job well, this aspect of the work easily ate up about 2 hours a day.
Look here. On the left, carefully encased in plastic, a letter from Le Président de la République française thanking me for my part in developing "Francophonie dans le monde." On the right, a Counseling Referral Form for Jesse ****** to Counselor Fortson:
As you probably can guess, nothing ever happened. Jesse was never tested for Learning Disabilities, never turned in a single assignment, continued to obstruct the classroom doorway, exacting a toll like some hulking Bridge Troll. His Mother and I chatted weekly, and she said the same thing at the end of every conversation, in that weird dissociative cheerful chirp: "Madame, what are we going to do about our Jesse?" I was feeling less and less like claiming the boy as he lost expensive textbooks, ruined class dynamics, and dragged his ass around my room, eating up the minutes of my 20-minute lunch break. "He stays in your room, Madame, because he likes you."
Madame was unable to find a single teacher who was passing Jesse but found great friends of Mother at every turn. She had so worked the teachers that some were unable to fail him for fear of Mother perhaps having another bad spell of high blood pressure. Any student who consistently receives a D is a student who really is failing but who has somehow struck a bargain, made a deal, or so terrified the prof by the prospect of repeating the course that they could pass it in absentia. By mid-semester, Jesse no longer had any textbooks to take home, or even put in his locker, as we each kept copies in class for him to not use. I made five photocopies of each cream, pink, and mint green triplicated version of his Deficiency Reports. He had his own section in my Telephone Log Book, and I even photocopied that, turning it in every Monday to the designated Vice-Principal and the aforementioned lazy ass Counselor Fortson.
If a student did not receive two successive Deficiency Reports, at least 6 weeks apart, that student could not be failed. Parents are supposed to sign them, return them, and work whatever plan is then imposed for turning the situation around.
Jesse had the brilliant idea of refusing to receive his Deficiency Reports. He would take it in hand, then drop it on the floor and abuse it with his large, floppy sneakers.
So I began taking pictures of him doing so, then retrieving my torn and smeared reports, encasing them in a sandwich baggy and mailing it to his Mom via registered mail. (You've no idea how much money a teacher ends up spending, nor the extents to which we will go to make sure students have what they need in terms of supplies.)
There was nothing wrong with Jesse beyond incredible obstinance. He was making his way through life by insinuating his bulk into doorways, blocking and tripping his Fellow Travelers, and being amused by it. I was several months into my new teaching venture before anyone explained the unusually high number of ill-prepared (read: couldn't read, write, or speak a word of French) advance students with which I was dealing. All I knew of the teacher I had replaced was that she had become ill. Apparently, she was terrified of the students, and fell prey to continual panic attacks at the mere hint of confrontation. The way it was eventually told to me, she failed to teach more than they failed to learn. Those who had her for their first year of foreign language were automatically advanced to the second year, where I was put in the position of correcting the "mistake." Those kids who fessed up to their inadequacies and put in time each week after school toward remediation, stayed, did their best, and passed, often with good marks. Those who decided that another year of playing the brute might pay off? They failed and were obnoxious about the whole affair. I tried to offer everyone who looked like they could use it an opportunity to start another foreign language (they could not repeat a course they had not failed) or find some different elective.
I failed Jesse. I had to work damned hard to do so, but I did it. Oh, the warm fuzzy feeling of that accomplishment by Madame! Oh, the looks of angry sadness from Jesse's Mom.
The Portfolio Committee made no commentary on the irony of my fierce achievements "to advance la francophonie in the world" versus my equally expansive failures with one Jesse ******.
Tucked in the back pocket of the portfolio is a "parent contact sheet."
Balancing all of that out are five pages of back-and-forth via email with the parents of one Albert d'H. I will never forget Albert d'H. He transfered as a ninth-grader from an exclusive private school (read: all white) to our "diverse urban high school." He had an extensive background in French and I had already been approached by his parents the week prior to school even starting because they were concerned he would be "bored." Apparently, he had never experienced instruction that was based in the target language, because when I interviewed him as part of the "warm up" to the course on Day 1, he burst into tears and ran into the hall. He was convinced that he was going to fail. I admit to having had little patience at being in the hall on the first day of class, being asked to promise someone that I "would not" fail him. His parents were so alarmed that they had him staying after school for tutorials 3-4 times a week. His father insisted on studying with him. The second week of school, his mother decided it was time for me to start preparing him for Junior Year Abroad. In fact, she was rapidly filling up every bit of free time the child might have between the ninth grade and his admission to law school.
She writes: "Älbert refuses to study with me so I have pretty much given up trying to follow what is going on in your class... I am writing now specifically to ask you if you know of any summer programs in France that would be suitable for Albert. I feel that full immmersion in French with supplementary grammar lessons would give him that boost he needs to start making real progress in learning the language. I would like to see him stay for at least six weeks or possibly eight. He's very stubborn, so I would like to send him to a really rigorous program where they would force him to work very hard. He needs it. I hope to hear from you soom and I appreciate all you have done in what must seem at times an impossible task."
It was not uncommon for me to be found mumbling, "poor Albert d'H, poor Albert d'H!"
As I sit here now, smiling at this collection of letters, forms, grades, deficiencies, and referrals, I can see all the faces, remember the laughter, and smile at the tears.
While I was out sick the last semester I taught there, I had the television tuned to a local channel. Spring had sprung and I was restless, anxious to get back to work. (I had broken a hip. Rather, a student had broken my hip by kicking and shoving a door I was trying to close -- he was being chased by cops in the hallway and sought refuge in my homeroom.)
The windows in our bedroom were open, I could hear birds and kids outside. Suddenly, the local news "sky cam" broke into the programming to share the feed of a high speed car chase down one of the highways... There were at least four cop cars wailing and weaving behind an old brown-and-white sedan with mismatched wheels.
I started to laugh.
I knew that car, I knew that silhouette!
That was one of my students!
It's as if I am reading the evidence of someone else's life. The memories stimulated by this odd group of documents are, for the most part, happy ones (with the exception of the remembered angst behind every asininely detailed "daily lesson plan"). Some of the entries are there solely to impress the committee evaluating educators by this "instrument." Some of the entries are there solely to irritate that same judgmental group -- like my inclusion of project guidelines for Throw-Away-the-Book Week.
There surely are things hinted at between the white vinyl covers that no sane person would miss. For example, I included the lengthy negative evaluation I received from an administrator who inspected one of my more advanced French classes. She gave me the lowest possible marks for stuff like clarity of instruction, review of home work assignments, and the flow of class exercises -- because all were conducted "in a foreign language," by far, the strangest criticism I ever received.
She was well-known for her negativity. When she came up to me at the close of class, she asked me why some assignment was not written on the board. I pointed out a boxed bit of writing in an upper corner and told her that that was the assignment (again, written in French), to which she responded with a doleful "I guess I have to take your word for it." I should have yelled: "Shazaam! You caught me pulling that old fake assignment trick. Foiled again!"
Okay, so as I tell you about The Portfolio, some of the old rigor returns. I am who I was; I remember me.
A big part of what The Bosses wanted to see involved student evaluations and evidence of "contact" with both student and parents/guardians. This aspect of teaching was really pretty new to me, as my experience until then was with college students. The onus of contact was more on the student in that world, though I did blur the directional road map when it seemed the right thing to do -- when someone was sick, depressed, or radically different from their norm. [This inclination was born with my very first batch of essays to grade. Near the top of the pile was an essay in the form of a suicide note. That surely cemented several good habits in me -- from attempting to return papers as fast as possible to cultivating a positive relationship with Campus Police. Incredibly, this happened once more in my career. How sad to think that I was their only available confidente.]
When I took a job at the high school level, I was clueless about the complexity of student/parent contact work. On paper, scheduling a 30-minute window for phone calls home and disciplinary referrals looked sufficient. In actuality, when I was doing my job well, this aspect of the work easily ate up about 2 hours a day.
Look here. On the left, carefully encased in plastic, a letter from Le Président de la République française thanking me for my part in developing "Francophonie dans le monde." On the right, a Counseling Referral Form for Jesse ****** to Counselor Fortson:
This referral results from observation of the following behaviors (followed by these checked items): Failure to complete work; Unable to pay attention; Disrupts class; Dazed or "spaced"; Inappropriate laughter; Short attention span; Hyperactive (restless, agitated); Overly talkative; Confused/Disoriented; Does not respond to questions; Sleepy/nods off in class; Isolated.
Action already taken by the classroom teacher making this referral:
Conferred with child on numerous occasions; Talked with parents on 9/7 and during visit to school the next week; According to Mother, Jesse was to have been tested for LD
Teacher Comments:
55 average. Often wanders around room. Gaining weight. Often blocks doorway during change of classes and refuses to move. Does virtually no work. I believe he was inadvertently passed in French 1 due to failure to issue deficiencies. He does not have requisite background to succeed in French 2. Mom and I have tried to work with him without success. Thank you.
As you probably can guess, nothing ever happened. Jesse was never tested for Learning Disabilities, never turned in a single assignment, continued to obstruct the classroom doorway, exacting a toll like some hulking Bridge Troll. His Mother and I chatted weekly, and she said the same thing at the end of every conversation, in that weird dissociative cheerful chirp: "Madame, what are we going to do about our Jesse?" I was feeling less and less like claiming the boy as he lost expensive textbooks, ruined class dynamics, and dragged his ass around my room, eating up the minutes of my 20-minute lunch break. "He stays in your room, Madame, because he likes you."
Madame was unable to find a single teacher who was passing Jesse but found great friends of Mother at every turn. She had so worked the teachers that some were unable to fail him for fear of Mother perhaps having another bad spell of high blood pressure. Any student who consistently receives a D is a student who really is failing but who has somehow struck a bargain, made a deal, or so terrified the prof by the prospect of repeating the course that they could pass it in absentia. By mid-semester, Jesse no longer had any textbooks to take home, or even put in his locker, as we each kept copies in class for him to not use. I made five photocopies of each cream, pink, and mint green triplicated version of his Deficiency Reports. He had his own section in my Telephone Log Book, and I even photocopied that, turning it in every Monday to the designated Vice-Principal and the aforementioned lazy ass Counselor Fortson.
If a student did not receive two successive Deficiency Reports, at least 6 weeks apart, that student could not be failed. Parents are supposed to sign them, return them, and work whatever plan is then imposed for turning the situation around.
Jesse had the brilliant idea of refusing to receive his Deficiency Reports. He would take it in hand, then drop it on the floor and abuse it with his large, floppy sneakers.
So I began taking pictures of him doing so, then retrieving my torn and smeared reports, encasing them in a sandwich baggy and mailing it to his Mom via registered mail. (You've no idea how much money a teacher ends up spending, nor the extents to which we will go to make sure students have what they need in terms of supplies.)
There was nothing wrong with Jesse beyond incredible obstinance. He was making his way through life by insinuating his bulk into doorways, blocking and tripping his Fellow Travelers, and being amused by it. I was several months into my new teaching venture before anyone explained the unusually high number of ill-prepared (read: couldn't read, write, or speak a word of French) advance students with which I was dealing. All I knew of the teacher I had replaced was that she had become ill. Apparently, she was terrified of the students, and fell prey to continual panic attacks at the mere hint of confrontation. The way it was eventually told to me, she failed to teach more than they failed to learn. Those who had her for their first year of foreign language were automatically advanced to the second year, where I was put in the position of correcting the "mistake." Those kids who fessed up to their inadequacies and put in time each week after school toward remediation, stayed, did their best, and passed, often with good marks. Those who decided that another year of playing the brute might pay off? They failed and were obnoxious about the whole affair. I tried to offer everyone who looked like they could use it an opportunity to start another foreign language (they could not repeat a course they had not failed) or find some different elective.
I failed Jesse. I had to work damned hard to do so, but I did it. Oh, the warm fuzzy feeling of that accomplishment by Madame! Oh, the looks of angry sadness from Jesse's Mom.
The Portfolio Committee made no commentary on the irony of my fierce achievements "to advance la francophonie in the world" versus my equally expansive failures with one Jesse ******.
Tucked in the back pocket of the portfolio is a "parent contact sheet."
URGENT: Spoke with Willie Edwards, father of Tracey Edwards. I called to inform of absence on 11-4 and continued failing grade. Tracey has also continued to interfere in communication between myself and parent/grandmother. Father said she had not returned home since morning of 11-3 and believes she has "run off with that boy" whom he describes as 18-19 with a criminal record. He asked that we keep an eye out for Tracey and that Mr. R, in particular, be notified. Requested contact by Mr. R. Mr. Edwards pager # is ***-***-****. He is very distraught.
Phone for Marco High disconnected. Called to report failure to serve detention, disruptive conduct, academic failure.
Spoke with mother of Jerry Hill. We will meet next Thursday. She was unaware of any progress reports from any teachers. Discussed failing grade, behavior. She said his father would address excessive talking and rude behavior with him. She was angry at not being called sooner.
Spoke with mother of C. Njoroge. He is currently failing French 2 -- very unexpected as he is generally excellent student. She says they are concerned at home. She said he is increasingly detached and perhaps is depressed. Mother notes a change since arrival in U.S. from Kenya last year. Fears negative peer pressure. Suggested tutorials. Will call father, per mother's request, in 2 weeks if no improvement noted. Mother stated very clearly that she wanted a referral to a counselor because she feels they are unable to communicate effectively with Chris.
Left message at ***-***-**** for Mrs. R, mother pf Lynneice R. I believe Lynneice picked up the phone initially, asked who it was, then hung up. When I called back, answering machine was on. Calling to schedule conference due to failure, cutting, poor class participation.
Received three phone calls to my home in one evening from Mr. S., father of students Kimberli and Kelli in advanced French 2. He has scheduled them for private music lessons and they both have several detentions to serve. They refuse to serve them before school and now are using the music lessons as an excuse to completely evade them. Mr. S was abusive and cursed at me repeatedly. I referred him to Mr. R and asked him to not contact me at home. Both girls were caught cheating on a quiz, both are missing whole chapters of assignments. Progress reports were sent home but Mr. S denies receiving them.
Scheduled meeting with grade-level counselor for Joyce R. and her mother. Joyce refused to take seat during class, paced the entire period, told me repeatedly, "I am going to take you out." She is exhibiting major mood swings, being friendly and cooperative one day, then argumentative and abusive the next. Mother said that I am a racist, that I did not understand the expression "I am going to take you out."
Balancing all of that out are five pages of back-and-forth via email with the parents of one Albert d'H. I will never forget Albert d'H. He transfered as a ninth-grader from an exclusive private school (read: all white) to our "diverse urban high school." He had an extensive background in French and I had already been approached by his parents the week prior to school even starting because they were concerned he would be "bored." Apparently, he had never experienced instruction that was based in the target language, because when I interviewed him as part of the "warm up" to the course on Day 1, he burst into tears and ran into the hall. He was convinced that he was going to fail. I admit to having had little patience at being in the hall on the first day of class, being asked to promise someone that I "would not" fail him. His parents were so alarmed that they had him staying after school for tutorials 3-4 times a week. His father insisted on studying with him. The second week of school, his mother decided it was time for me to start preparing him for Junior Year Abroad. In fact, she was rapidly filling up every bit of free time the child might have between the ninth grade and his admission to law school.
She writes: "Älbert refuses to study with me so I have pretty much given up trying to follow what is going on in your class... I am writing now specifically to ask you if you know of any summer programs in France that would be suitable for Albert. I feel that full immmersion in French with supplementary grammar lessons would give him that boost he needs to start making real progress in learning the language. I would like to see him stay for at least six weeks or possibly eight. He's very stubborn, so I would like to send him to a really rigorous program where they would force him to work very hard. He needs it. I hope to hear from you soom and I appreciate all you have done in what must seem at times an impossible task."
It was not uncommon for me to be found mumbling, "poor Albert d'H, poor Albert d'H!"
As I sit here now, smiling at this collection of letters, forms, grades, deficiencies, and referrals, I can see all the faces, remember the laughter, and smile at the tears.
While I was out sick the last semester I taught there, I had the television tuned to a local channel. Spring had sprung and I was restless, anxious to get back to work. (I had broken a hip. Rather, a student had broken my hip by kicking and shoving a door I was trying to close -- he was being chased by cops in the hallway and sought refuge in my homeroom.)
The windows in our bedroom were open, I could hear birds and kids outside. Suddenly, the local news "sky cam" broke into the programming to share the feed of a high speed car chase down one of the highways... There were at least four cop cars wailing and weaving behind an old brown-and-white sedan with mismatched wheels.
I started to laugh.
I knew that car, I knew that silhouette!
That was one of my students!
_1.jpg)





{kind=link}
{kind=link}
{kind=link}
{kind=link}